BAC March Slide Club review
Case 1: EGFR-Mutant Lung Adenocarcinoma with Small Cell Transformation
Presenter: Anthony Maddox
Patient: 80-year-old woman
Presentation: Persistent cough and mild weight loss
Smoking history: 10 pack years
Initial Findings
- Left hilar mass with nodal enlargement on imaging
- EBUS FNA performed
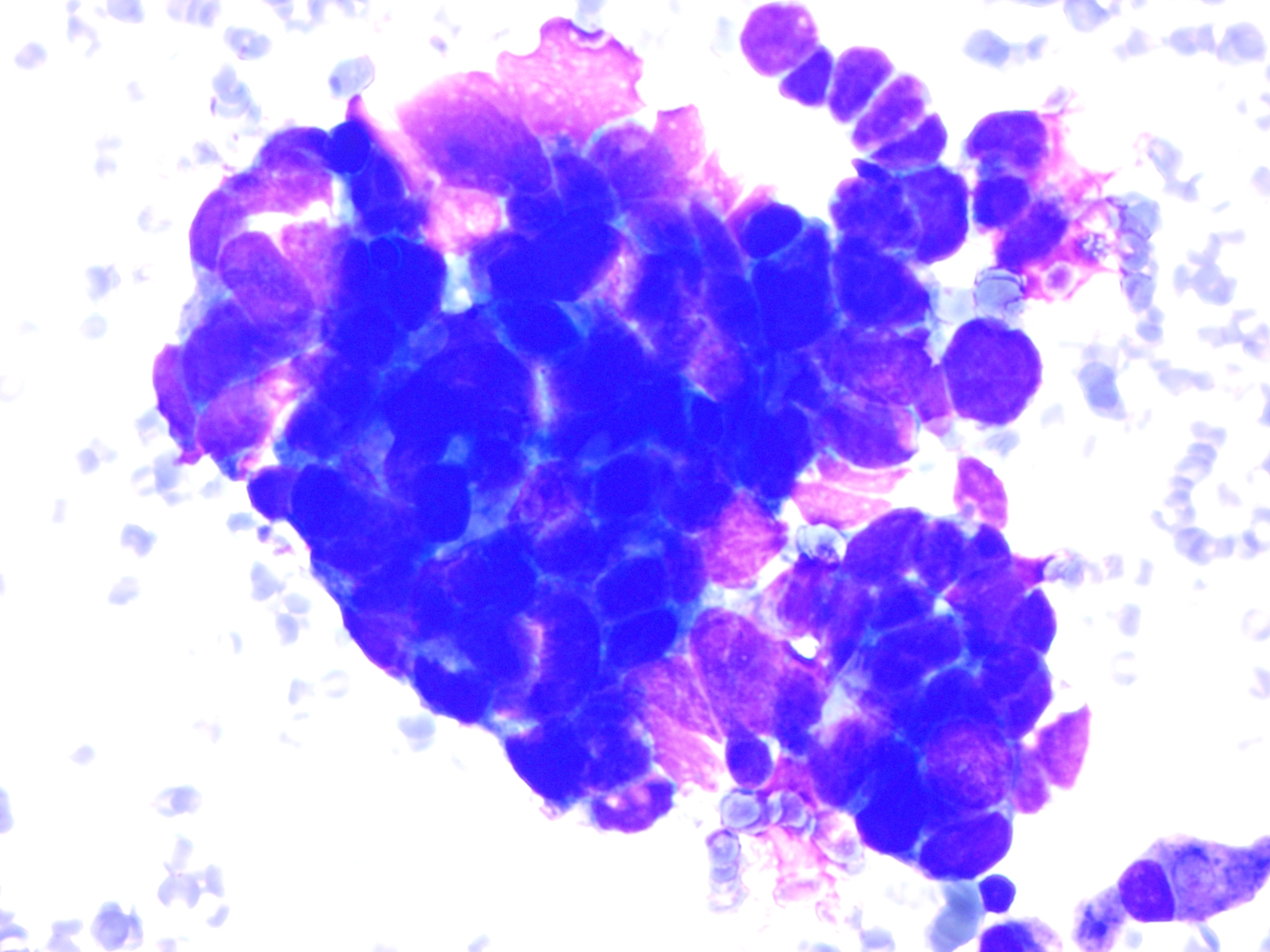
Cytology (EBUS)
- Highly cellular sample
- Pleomorphic epithelial cells
- Abundant cytoplasm
- Features consistent with non-small cell carcinoma
- Cell block showed glandular architecture
Immunohistochemistry: TTF-1 positive
Diagnosis: Lung adenocarcinoma
Molecular testing: EGFR L858R mutation detected
Treatment
- Started on osimertinib (EGFR tyrosine kinase inhibitor)
- Initial clinical response
Disease Progression (8 Months Later)
- Worsening breathlessness
- Large pleural effusion
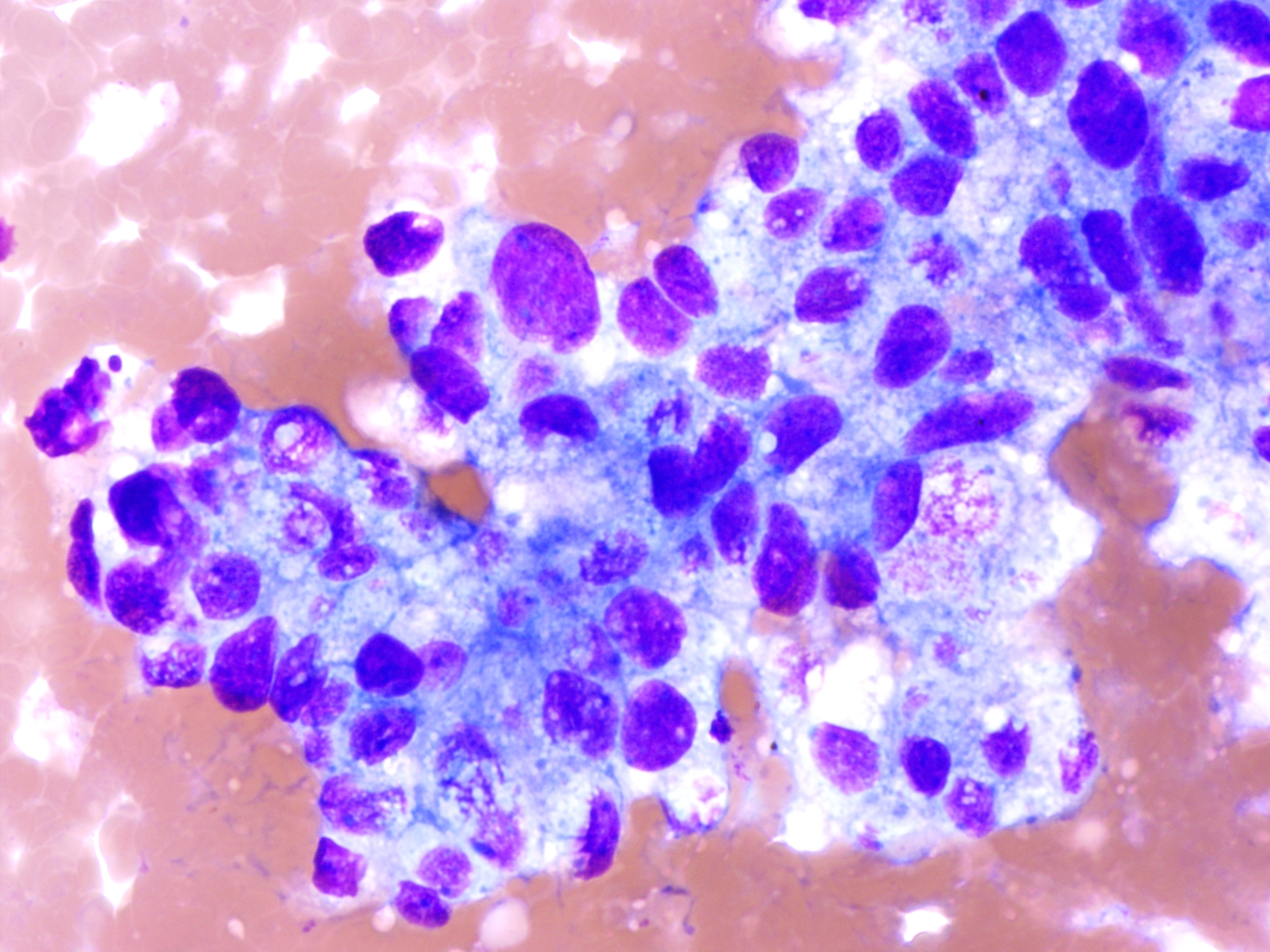
Pleural Fluid Cytology
- Reactive background
- Small clusters of atypical cells
- High N:C ratio
- Nuclear moulding
- Finely granular chromatin
Immunohistochemistry:
- Cytokeratin positive
- TTF-1 positive
- Synaptophysin positive
- CD56 positive
- Chromogranin negative
Final Diagnosis: Small cell carcinoma following EGFR TKI therapy
Key Learning Points
- EGFR-mutant adenocarcinomas can transform to small cell carcinoma under TKI pressure
- Transformation is a recognised resistance mechanism
- Cytological features may be subtle and easily overlooked
- Clinical context is essential
Outcome: Patient died approximately six months after transformation
Case 2: Peritoneal Fluid – Low Grade Serous Carcinoma
Presenter: Leonie Wheeldon
Patient: 55-year-old woman
Presentation: Abdominal pain
History: Endometriosis
Imaging: 5 cm right ovarian mass
CA-125: 70
Specimens
- Peritoneal fluid
- Peritoneal washings
Cytology Findings
- Papillary epithelial groups
- Numerous psammoma bodies
- Mild-to-moderate nuclear atypia
- Relatively uniform nuclei
- Smooth nuclear contours
- Discrete nucleoli
Immunohistochemistry
- BerEP4 positive
- Calretinin negative
- PAX8 positive
- WT1 positive
- CK7 positive
- CK20 negative
- CDX2 negative
- p53 wild-type pattern
Final Interpretation: Low grade serous carcinoma (ovarian origin)
Key Learning Points
- Psammoma bodies favour low grade serous carcinoma
- Nuclear features are critical in grading
- p53 wild-type pattern supports low grade disease
- Cytology alone may overcall high grade carcinoma
- Histology correlation is essential when features are borderline
Practical Reporting Advice
- Avoid over-calling grade when cytology is equivocal
- Correlate with MDT discussion and surgical findings
- Await histology where necessary
Session Summary
This session highlighted tumour evolution under targeted therapy, diagnostic pitfalls in fluid cytology, the importance of nuclear assessment, and the value of clinicopathological correlation.